
Editor's Choice
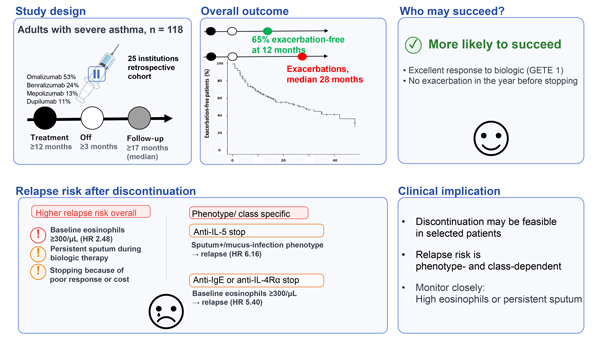
Editor’s comment: Biologics are highly effective in severe asthma—but can they be safely discontinued? In this retrospective study of 118 patients, Nagasaki et al. (Japan) reported that approximately 65% remained exacerbation free 12 months after stopping treatment. Patients with a strong treatment response and no recent exacerbations were more likely to discontinue successfully. In contrast, baseline eosinophilia, persistent sputum symptoms, and discontinuation due to poor response or cost were associated with relapse, with some variation across biologic classes. These findings suggest that discontinuation is feasible in carefully selected, well-controlled patients.
On non-biologic treatment clinical remission in adult-onset asthma: A 20-year cohort study in Taiwan
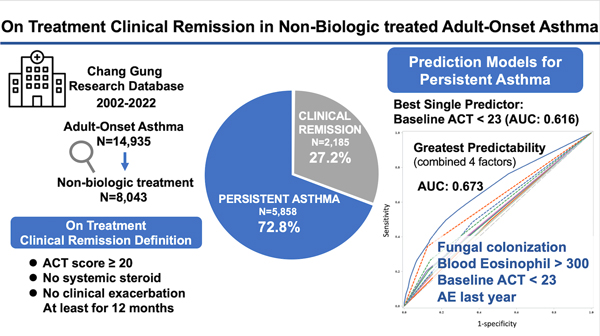
Editor’s comment: How often can asthma patients achieve remission without biologics? In a large real-world cohort spanning 20 years, Lin et al. (Taiwan) retrospectively analyzed the records of 8,043 adults and found that 27% achieved remission—defined as good symptom control, no systemic steroid use, and no exacerbations for ≥12 months. Persistent disease was associated with smoking, impaired lung function, eosinophilia, fungal colonization, poor baseline symptom control, and recent exacerbations. Among these, poor baseline symptom control emerged as the strongest predictor of failure to achieve remission. These findings indicate that remission is achievable with standard therapy—and that simple clinical markers can help identify patients unlikely to reach it.
This data-driven approach helps clarify which allergens drive each person's allergic reactions.
Review Series: Cytokines as therapeutic targets: Insights from clinical interventions
The advent of molecularly targeted therapies has fundamentally changed our understanding of allergic diseases. Beyond expanding treatment options, these therapies allow us to explore human disease in vivo by selectively targeting a single molecule and clarifying its role within complex immune networks. We hope that this series will offer useful insights for clinicians and researchers, serving as a reminder that the results of therapeutic intervention can help elucidate the fundamental biology of allergic disease.
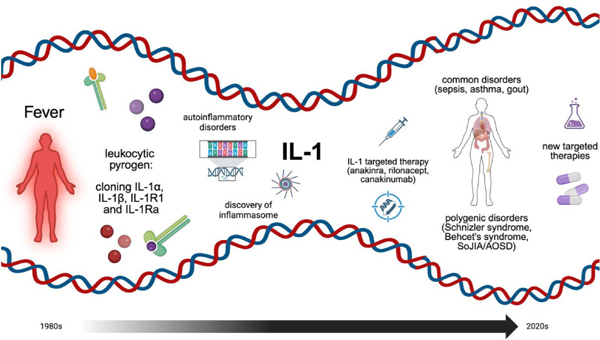
Broderick et al. provide an overview of the history of IL-1 research, its molecular mechanisms, and its relevance as a therapeutic target.
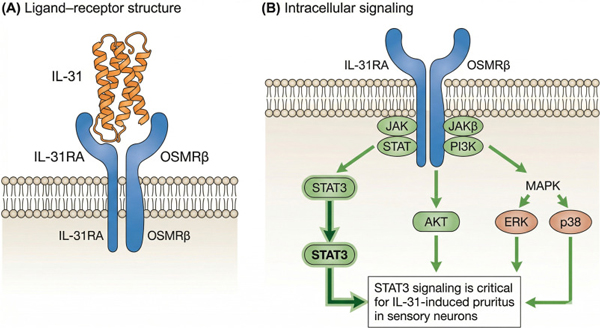
Irie et al. summarize our current knowledge of IL-31, including its cellular sources, receptor distribution, and its role in neuro–immune interactions.
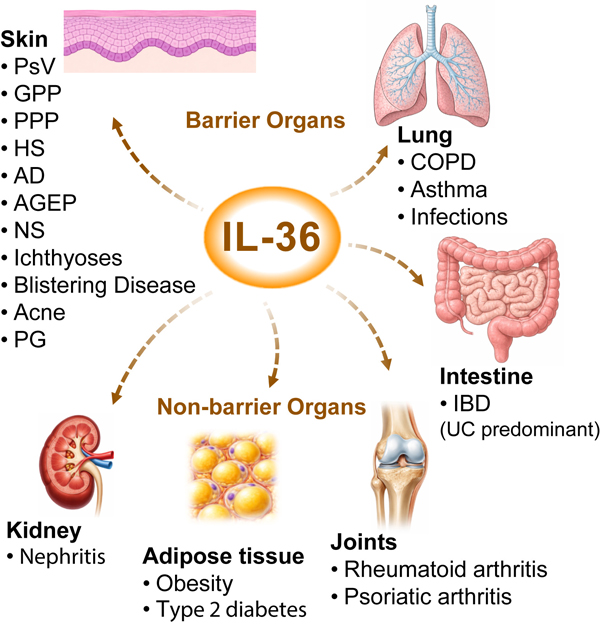
Satoh et al. offer a comprehensive overview of the molecular biology of IL-36, its signaling pathways, and its clinical relevance.